

Treatments vs. Skincare: What the Bathroom Can and Cannot Replace
A clear distinction between what clinical treatments change, what skincare can maintain, and where beauty marketing deliberately blurs the line.

There are things a clinic can do that your bathroom cannot replicate.
This is physiology, not opinion. Botulinum toxin cannot be copied by a peptide cream. Filler cannot be replaced by a topical serum. Deep resurfacing and controlled injury cannot be replicated by a product that sits on the surface of intact skin. The mechanisms are entirely different, and the outcomes, however convincingly described in product marketing are not equivalent.
The honest question is not whether skincare can replace the clinic. Most people already know, if they are honest with themselves, that it cannot, not for the outcomes the clinic produces. The honest question is where skincare is genuinely enough, and where pretending it is enough becomes expensive, and occasionally harmful, misinformation.
That question is worth answering carefully.
The beauty industry has a consistent interest in not answering it at all, because the answer requires distinguishing between categories of product some of which have meaningful evidence behind their claims, and some of which do not, and that distinction is commercially inconvenient in a market where the premium serum and the evidence-backed treatment often share a shelf and a price point.
This essay makes the distinction.
It is the essay the industry prefers not to publish.

What the Clinic Actually Does
Understanding the gap between clinic and bathroom requires a clear account of what clinical treatments actually do, not in the language of marketing, but in the language of mechanism.
The distinction begins with depth: how far into the skin or tissue the intervention can act, and what biological mechanism it is designed to trigger.
Botulinum toxin — Botox and equivalent products temporarily reduces the nerve signalling that causes specific muscles to contract. The result is a reduction in the movement that creates dynamic lines. The effect is specific, measurable, and determined by the injection site, depth, dilution, and quantity administered.
No topical product produces this mechanism.
Products marketed as “Botox alternatives” operate through entirely different pathways usually surface hydration, temporary tightening, light-reflecting finish, or very mild effects on expression-related appearance. Some may make the skin look smoother. Some may soften the appearance of lines temporarily. But they do not interrupt muscle contraction in the way botulinum toxin does.
They are not alternatives.
They are different products.
Dermal fillers add temporary physical volume or contour to specific structural areas. Hyaluronic acid fillers are placed beneath the skin or within deeper tissue planes, where they can restore volume, soften folds, or alter contour depending on product choice and injection technique.
The hyaluronic acid in a topical serum or cream does not do this.
Topical hyaluronic acid can bind water and improve surface hydration. That matters. It can make the skin look fresher, smoother, and more comfortable. But it cannot create cheek structure, replace lost facial fat, lift a fold, or restore volume from beneath the skin. The two products share an ingredient name. They do not share a mechanism or an outcome.
Laser resurfacing and professional peels work through controlled injury: the deliberate disruption of the skin’s surface, or deeper layers depending on the procedure, in a way that triggers repair and remodelling. The depth and precision of the injury determine the outcome. These are procedures with recovery periods because they are, in a specific technical sense, wounds — managed, calibrated, therapeutically intended wounds.
The “at-home peels” and “resurfacing serums” available over the counter operate at concentrations and depths that cannot replicate this mechanism without producing outcomes that would not be appropriate or legally permissible in a consumer product.
Microneedling creates controlled micro-injuries in the skin. These serve two functions: they stimulate a wound-healing response and, depending on protocol, may increase the penetration of certain products applied around the treatment window.
The controlled injury is the point.
This is categorically different from applying the same actives to intact skin.
It is also precisely why microneedling should be performed by qualified practitioners under appropriate hygiene and safety conditions, not treated as an aggressive home experiment. The issue is not simply whether the device creates holes in the skin. It is whether those injuries are controlled, sterile, appropriate to the skin, and managed correctly before and after treatment.
Clinical treatments are not more serious because they are more expensive.
They are more serious because they intervene differently.
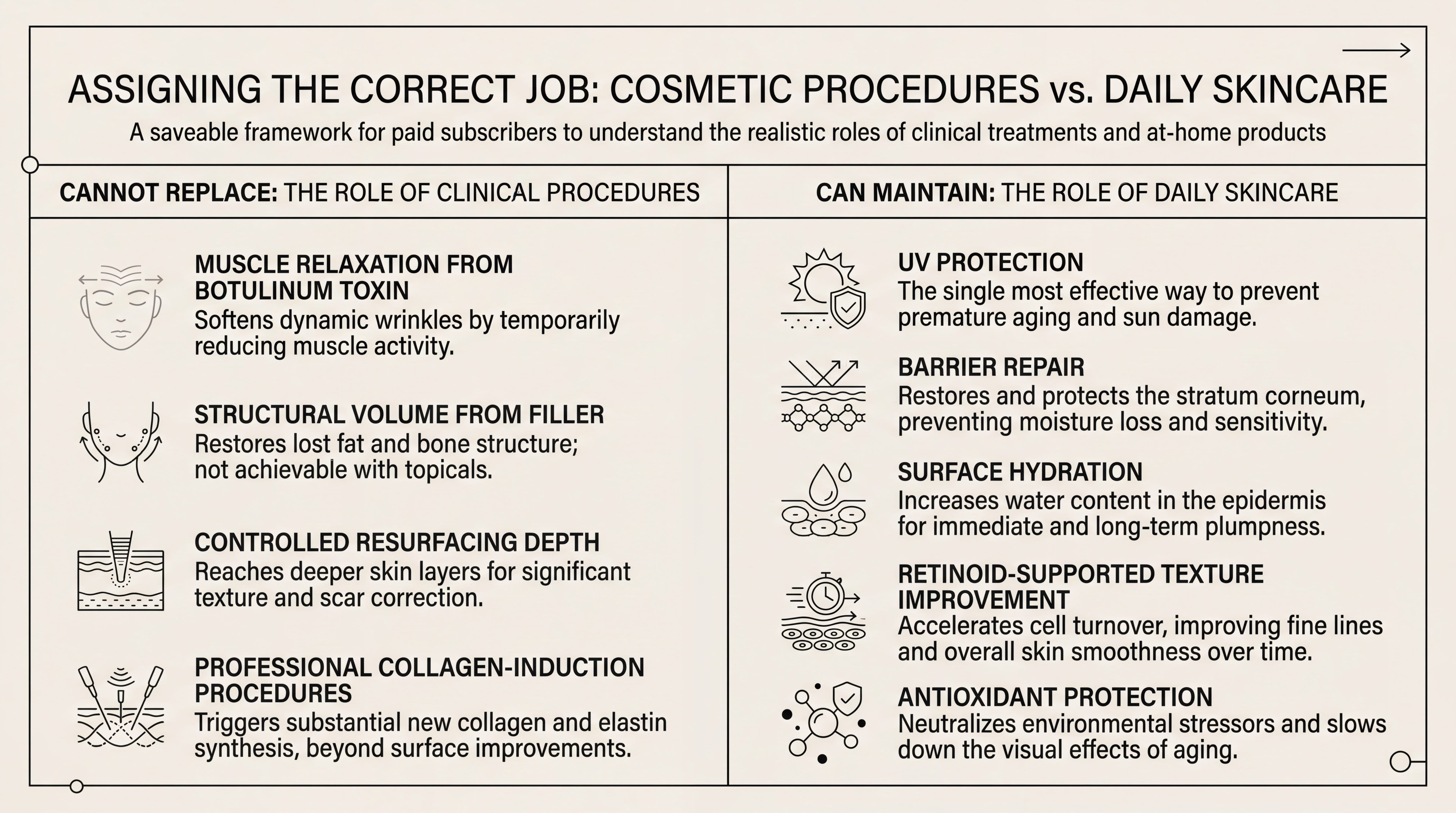
What Skincare Can Maintain
The above section is not an argument that skincare is ineffective.
It is an argument for precision.
Skincare can do specific things very well. The error and it is a structurally encouraged error is conflating “does something” with “does the same thing as a clinical treatment.”
Here is what the evidence and mechanism support.
Antioxidant protection notably vitamin C, often formulated with vitamin E and ferulic acid addresses some of the environmental stressors that clinical treatments often correct after the fact. The logic is prevention and support rather than dramatic reversal. L-ascorbic acid at an effective concentration, usually between 10 and 20 percent depending on formulation and tolerance, can help reduce oxidative stress from UV exposure and pollution.
This does not reverse existing photodamage at the level a laser can address.
It reduces the rate at which new damage accumulates.
Different mechanism. Different timeline. Still genuinely useful.
Barrier repair — ceramides, fatty acids, cholesterol, niacinamide, and appropriate occlusives — is one of the most important functions in topical skincare and one of the most consistently undervalued. A compromised barrier allows transepidermal water loss to increase, which can create a cycle of dryness, sensitivity, irritation, inflammation, and poor tolerance to actives.
Repairing the barrier with correctly formulated products is not glamorous in the way a peel or injectable is glamorous.
But it is foundational.
A skin barrier that is functioning well determines how much the skin can tolerate, how quickly it recovers, how well it responds to actives, and how long it can maintain clinical results without tipping into irritation.
Surface hydration — multi-weight hyaluronic acid, panthenol, glycerin, beta-glucan, urea in appropriate concentrations produces visible effects on plumpness, texture, and comfort at the surface level.
These are not the same as structural volume added by injectable filler.
They are genuine hydration effects that have meaningful impact on how skin appears in the short and medium term. The products are legitimate. The claims should be proportionate.
Retinoids — vitamin A derivatives including retinol, retinaldehyde, adapalene in some markets, and prescription-strength tretinoin have one of the strongest long-term bodies of evidence in topical anti-ageing skincare. They can support cell turnover, improve uneven texture, help with some pigmentation patterns, and stimulate collagen-related changes over time.
The caveat is important: the evidence is strongest for prescription retinoids such as tretinoin. Over-the-counter retinol and retinaldehyde can produce real effects, but usually more slowly and with more modest results.
A retinoid is not a laser.
It is not filler.
It is not botulinum toxin.
It is a long-term topical discipline.
Sunscreen — broad-spectrum SPF used daily is the single highest-impact skincare decision available. The evidence for daily photoprotection in preventing photodamage and premature skin ageing is strong and consistent. No serum, acid, cream, or facial device can compensate for unprotected UV exposure.
In high-UV climates, after procedures, during pigmentation treatment, or when using retinoids and acids, SPF becomes even less negotiable.
This is the least exciting advice in beauty.
It is also the advice with the highest return.

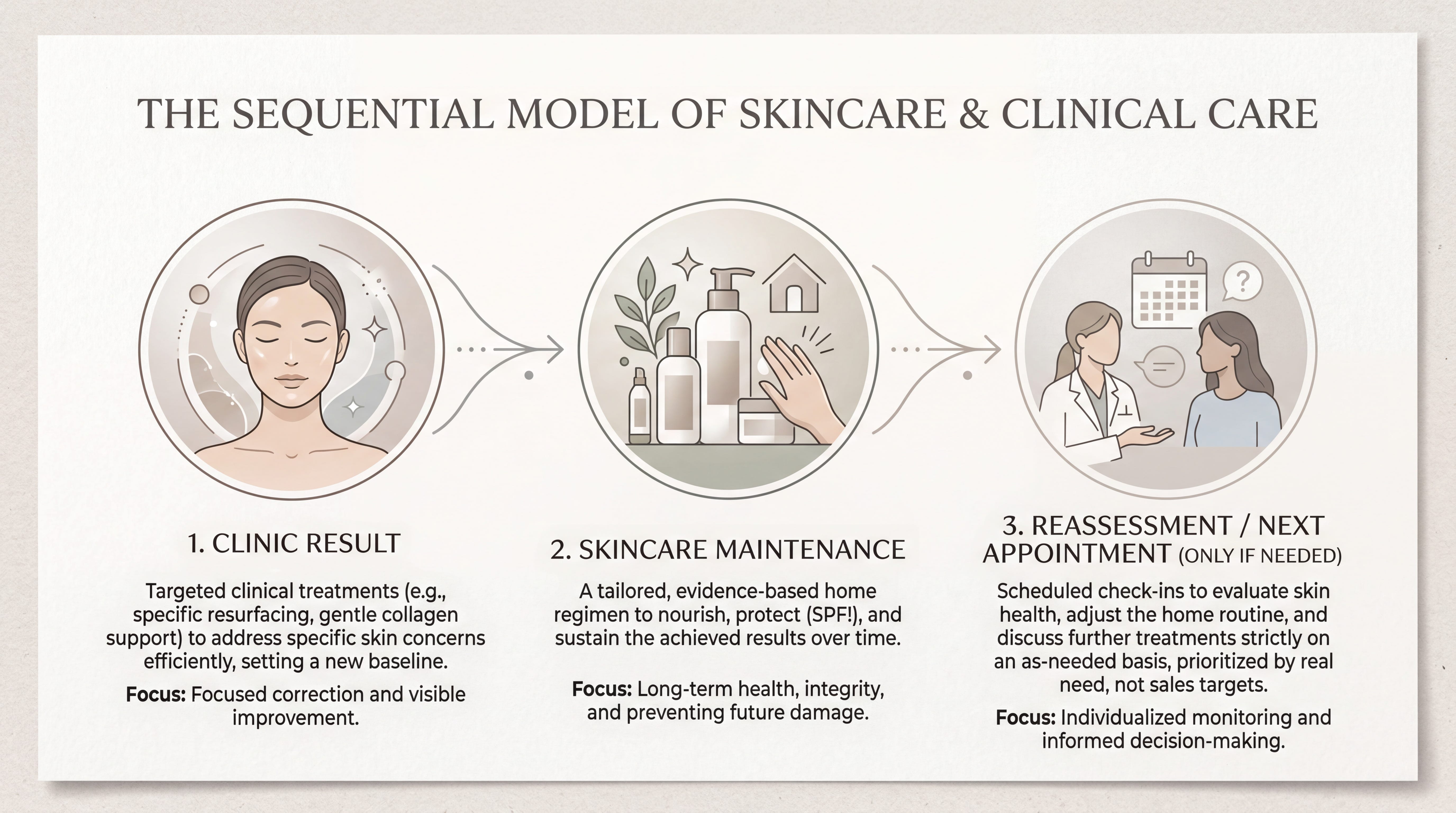
The Sequencing Framework
The most useful way to think about clinic and skincare is not either/or.
It is sequential.
Phase One: Establish the Routine
Before any clinical investment makes sense, the foundational skincare routine should be working: effective cleansing, antioxidant protection in the morning if tolerated, barrier support, retinoid in the evening if appropriate, and daily SPF.
These decisions do not produce dramatic before-and-after photographs.
They produce a baseline of skin health.
That baseline determines how well clinical treatments work, how safely the skin tolerates them, and how long their outcomes last.
A laser performed on skin with an impaired barrier is not the same experience as a laser performed on skin that is stable, protected, and well maintained. Filler placed into a face whose skin is chronically inflamed, dehydrated, or sun-damaged may still create volume, but it will not solve the broader quality problem. Botulinum toxin may soften dynamic lines, but it will not make dull, irritated, unprotected skin look healthy by itself.
The bathroom cannot replace the clinic.
But the clinic cannot compensate for a neglected bathroom either.
Phase Two: Assess the Concern
Not all skin concerns require clinical intervention.
Surface-level hyperpigmentation, mild texture irregularity, dehydration, barrier damage, early fine lines, and dullness may respond meaningfully to evidence-based topical routines over time.
Deeper structural concerns - volume loss, significant laxity, persistent dynamic lines, deeper folds, severe photodamage, acne scarring, or pronounced pigmentation patterns, usually require professional assessment and, in some cases, clinical intervention.
The distinction matters because the wrong category wastes money.
Buying a serum for structural volume loss is expensive denial.
Booking a procedure for a barrier problem is expensive impatience.
Both mistakes are common.
Phase Three: Use Skincare to Maintain Clinical Outcomes
This is where the relationship between the two categories becomes genuinely efficient.
A well-conducted laser treatment maintained with daily SPF, antioxidants, and barrier support will almost always make more sense than a laser treatment followed by inconsistent protection and aggressive actives.
A filler appointment maintained with healthy skin, stable hydration, and good photoprotection will usually look better than the same appointment sitting beneath irritated, inflamed, neglected skin.
Botulinum toxin may reduce movement, but the skin over that movement still needs care.
Clinical treatment and skincare are most effective as a system, not as competing options.
Where the Money Disappears
The most expensive mistakes in beauty rarely look irrational at the moment they are made.
They look like hope.
A person notices a change in their face a line, a hollow, a patch of pigmentation, a new looseness in the lower face, a texture that no longer behaves under makeup and buys the thing that promises the least frightening solution. A serum feels safer than a consultation. A cream feels more private than a procedure. A product can be purchased quietly, used at home, and believed in without anyone else assessing the concern too directly.
This is how bathroom spending becomes expensive.
Not because skincare is useless.
Because it is often being asked to do the wrong job.
The premium cream bought for sagging skin is not really a cream purchase. It is an attempt to avoid the possibility that the concern is structural. The peptide serum bought as a “needle-free Botox” is not really a peptide purchase. It is an attempt to treat movement without intervening in movement. The hydrating mask bought for facial volume loss is not really a hydration purchase. It is a wish that surface plumpness might behave like architecture.
The product may be beautifully formulated.
The category may still be wrong.
This is the distinction that saves money: before asking which product is best, ask what kind of problem you are trying to solve.
Is the problem movement? That is not a cream problem.
Is the problem volume? That is not a serum problem.
Is the problem pigmentation? It depends, because pigment can be epidermal, dermal, hormonal, inflammatory, sun-driven, or mixed. Some forms respond to topical routines; others require prescription treatment, lasers, peels, or a long-term management plan.
Is the problem dullness? That may be topical.
Is the problem barrier damage? That is almost certainly not solved by adding more actives.
Is the problem texture? Maybe. The word texture covers too much territory. Congestion, dehydration, scars, enlarged pores, fine lines, roughness, and post-inflammatory change are not the same concern, even though beauty marketing frequently sells them under the same promise.
This is why diagnosis matters.
Not diagnosis in the dramatic sense. Diagnosis in the practical sense: identifying what category the concern belongs to before spending against it.
The beauty industry profits from category confusion because confusion increases purchasing frequency. If the consumer does not know whether the problem is structural, inflammatory, pigmentary, muscular, vascular, or barrier-related, she can be sold almost anything that uses the right language. Firming. Plumping. Resurfacing. Lifting. Smoothing. Brightening. Repairing. Rejuvenating.
These words are not meaningless.
But they are often imprecise.
A good beauty routine begins when the words become specific enough to be useful.
The second place money disappears is duplication. Three hydrating serums doing the work of one. Multiple acids used in rotation by a skin barrier that wanted none of them. A retinol, a retinal, an exfoliating toner, and a “resurfacing” mask all competing for the same irritated face. A moisturiser bought for every mood rather than every need.
More products do not create a more serious routine.
A serious routine is one where every product has a job.
The third place money disappears is impatience. Evidence-based skincare takes time. Retinoids need months, not days. Pigmentation management is slow. Barrier repair requires subtraction as much as addition. SPF prevents more dramatically than it reverses. A product abandoned after two weeks may not have failed; it may never have been given the timeline its mechanism requires.
But the opposite is also true.
A product used faithfully for a year against the wrong category of concern has not been patient skincare. It has been delayed clarity.
This is the paid lesson: spend first on understanding the category of the concern. Then spend on the appropriate intervention.
The cheapest mistake is usually the product you do not buy because you finally understand what it could never have done.
Product Categories to Understand
Vitamin C Serums
Look for L-ascorbic acid if your skin can tolerate it, usually in the 10–20 percent range depending on the formulation. Vitamin C is unstable, so packaging matters. Light, air, and heat can degrade the formula. Opaque or air-restricted packaging is a quality signal.
Vitamin C is not a laser. It is antioxidant support.
Niacinamide
Niacinamide is useful for barrier support, uneven tone, visible redness in some skin types, and oil regulation. A 4–5 percent concentration is often enough. Higher is not automatically better, and some people flush or become irritated at higher concentrations.
Niacinamide is one of the better examples of a non-dramatic ingredient that earns its place through usefulness rather than theatre.
Retinoids
Start lower than you think you need to and increase slowly.
The irritation that comes from introducing a retinoid too quickly can undo the benefit by damaging the barrier and creating inflammation. Tretinoin, where appropriate and prescribed, remains the standard against which many topical anti-ageing claims are measured. Retinol and retinaldehyde can still be meaningful, but they require patience.
A retinoid routine is not a personality test. It is a tolerance strategy.
SPF
Mineral or chemical — the distinction matters less than daily consistent application, broad-spectrum protection, and whether the formula suits your skin well enough that you will actually wear it.
The best SPF is the one that sits well enough on your skin that you apply it every morning without negotiating with yourself about whether today counts as a sun-exposure day.
In beauty, consistency beats theoretical superiority almost every time.
The Honest Decision Tree
Is the concern structural volume loss, significant sagging, deep folds, or persistent dynamic lines?
Skincare will not meaningfully address this. A professional consultation is appropriate.
Is the concern surface-level mild texture, dullness, dehydration, early fine lines, or mild pigmentation?
Evidence-based skincare may have meaningful interventions here. Establish the routine and assess over 12–16 weeks before escalating, unless the concern is severe, worsening, or medically suspicious.
Have you established a basic routine with SPF, barrier support, and an appropriate active?
If not, begin there. Clinical treatments on a compromised baseline often produce less elegant and less durable outcomes.
Is the concern primarily about maintenance of a clinical result?
This is the highest-value use of skincare. The SPF that maintains the laser result. The barrier-repair routine that supports post-treatment recovery. The retinoid that improves texture over time. The antioxidant that reduces new environmental damage accumulating.
Are you considering a clinical procedure without having consulted a qualified dermatologist or aesthetic practitioner?
Do that first.
The internet, including this essay, cannot replace that assessment.
The Real Distinction
This is not anti-skincare.
It is not pro-clinic.
It is anti-confusion.
The most intelligent beauty routine is not the one that rejects the clinic or the one that treats skincare as decorative maintenance. It is the one that understands sequence, mechanism, and proportion.
The bathroom is powerful when it is asked to do the work it can actually do.
The clinic is valuable when it is used for concerns the bathroom was never built to solve.
Confusing the two is where the money disappears.
And in beauty, clarity may be the most expensive-looking thing a person can have.
Medical disclaimer: This essay is editorial content and does not constitute medical advice. All clinical decisions should be made in consultation with a qualified dermatologist, doctor, or aesthetic medicine practitioner.